Ultrasound Equipment
Beyond the darkened suite – Ultrasound becomes the frontline brain of modern medicine

Ultrasound once confirmed others’ findings; now it leads urgent decisions, reinvented from grayscale sidekick to intelligent clinical platform.

Walk into a busy emergency department today and ultrasound no longer sits in the wings. It glides between trauma bays and resuscitation rooms, switching from abdomen to heart to lungs without leaving the patient’s side. A generation ago, it largely followed other imaging; now, it often sets the diagnostic agenda. Its appeal is simple yet powerful – real-time visualization, no ionizing radiation, and the ability to travel wherever the patient is rather than summoning the patient to where the machine lives.
This migration from radiology suite to frontline has reshaped clinical habits. Instead of postponing decisions until the scan is back, clinicians frame their thinking around questions ultrasound can answer now: Is there free fluid? Is the heart failing? Is the foetus at risk? Bedside images become a living extension of the physical exam, collapsing the distance between suspicion and certainty. What once felt like a test is increasingly experienced as a conversation between clinician, patient, and machine.
The tone of that conversation is changing too. The grainy, operator-dependent images of old are giving way to crisp, consistent views powered by advances in transducers, signal processing, and software. Paired with portable and handheld devices, ultrasound has escaped the gravity of fixed infrastructure. From intensive care units and operating rooms to ambulances and rural outposts, it follows the patient’s journey rather than interrupting it.
Physics, transducers, and the hidden engine of change
Behind this transformation lies a story of physics quietly rewritten. Ultrasound has always relied on acoustic waves and impedance matching, yet the past two decades have pushed those principles to new extremes. Materials science and microfabrication have turned once-bulky piezoelectric ceramics into refined composites, CMUTs, and PMUTs–transducers that steer beams with surgical precision, stretch bandwidth, and sharpen both axial and lateral resolution. These innovations have made it possible to see deeper, clearer, and more reliably than before.
Signal fidelity, long constrained by reflection and noise, has been steadily reclaimed. Sophisticated acoustic coupling layers and frequency-adaptive pulses coax more information from every echo. Techniques such as coherent compounding, plane-wave imaging, and ultrafast Doppler stack wavefronts like pages in a book, revealing microvascular flow or subtle tissue motion that older systems simply missed. The result is not just a prettier picture; it is a richer narrative about how tissues behave, perfuse, and fail.
Penetration, too, has broken free of old trade-offs. By dynamically adjusting frequency, pulse length, and power, modern beamforming balances deep reach with fine detail–even across patients with very different body habitus. Adaptive attenuation compensation helps preserve a consistent experience from one individual to the next. On top of this physics platform, new modalities–photoacoustic imaging, elastography, and emerging wearables–are stretching ultrasound beyond structure to function, biomechanics, and even early molecular signatures. What used to be a snapshot is gradually turning into a multiparametric biography of the patient’s physiology.
A market that mirrors a clinical shift
Markets tend to move where clinical practice is already headed, and ultrasound is no exception. The global ultrasound equipment market is estimated at USD 10.69 billion in 2025 and is projected to grow from USD 11.58 billion in 2026 to USD 23.71 billion by 2035, at a CAGR of 8.29 percent between 2026 and 2035, according to Precedence Research. That growth narrates a story: an aging world grappling with chronic disease, health systems pressed to do more with less, and clinicians demanding tools that are both powerful and portable.
Governments have quietly become co-authors of this story. Policy pushes for early cancer detection, maternal and foetal health, and preventive cardiology have elevated ultrasound from nice to have to non-negotiable in many national programs. Expanded public spending, better reimbursement for non-invasive diagnostics, and support for equipment upgrades have encouraged hospitals and clinics to rethink their imaging mix. In emerging markets, where CT and MRI remain scarce, ultrasound often emerges as the first scalable diagnostic backbone.
The trajectory is not without turbulence. High upfront costs, recurring maintenance, and chronic shortages of trained sonographers and radiologists slow adoption, particularly outside urban centers. Competing imaging modalities–CT, MRI, and even AI-enhanced x-ray–vie for budget and attention. Yet the long arc bends unmistakably toward ultrasound. As therapeutic applications mature and AI pushes performance further, ultrasound’s role broadens from image generator to clinical engine, anchoring value in outcomes rather than machines.
Indian market dynamics
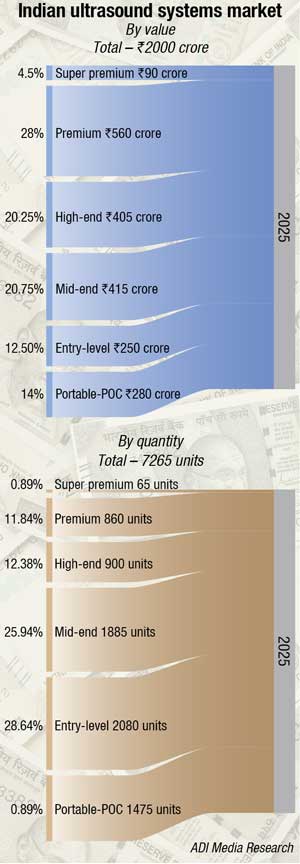
The Indian ultrasound systems market is estimated at ₹2000 crore in 2025.
GE HealthCare commands a significant share, followed by Mindray and Samsung. GE sold about 50 units in 2025, with each system priced at roughly ₹1.5 crore, according to industry estimates. GE’s premium platforms, including the Voluson Expert 22 and the newer Signature 20 and 18 systems, widely recognized for their advanced 3D/4D imaging and AI-enabled workflows, have been key contributors to this performance.
| Leading players – Indian ultrasound systems market* 2025 |
|
| Tier I | GE |
| Tier II | Mindray, and Samsung |
| Tier III | Fujifilm Sonosite, Philips, and BPL |
| Others | Siemens, Konica, Esaote, Toshiba, Aloka, Fujifilm, Edan, Chison, and Cura |
|
*Vendors are placed in different tiers on the basis of their sales contribution to the overall revenues of the Indian ultrasound systems market. ADI Media Research |
|
In the refurbished segment, aggressive buyback-driven activity and the entry of Chinese manufacturers such as Chison, Zoncare, VINNO, and Wisonic have reshaped the low-end market, where GE has ceded share at the entry level to Mindray and Samsung.
Radiology still dominates installed ultrasound capacity, but the fastest growth is coming from critical care and emergency settings, where point-of-care protocols are being woven into sepsis bundles, trauma pathways, and perioperative workflows. Portable and compact systems–often procured through state health schemes, CSR funding, and NGO partnerships–are emerging as the de facto imaging backbone for district hospitals and community health centres, particularly for maternal and child health, tuberculosis, and non-communicable disease screening. Policy pushes under the National Health Mission and Ayushman Bharat, together with expanding telemedicine pilots, are steadily nudging ultrasound out of metropolitan hubs into Tier-II cities and rural belts, where handheld and trolley-based POCUS platforms are increasingly the first–if not the only–imaging touchpoint.
Vendors are pivoting from product-centric to solution-centric playbooks, and that shift is most visible in how they design, price, and support systems across sharply differentiated tiers of care. Global OEMs now approach India with tiered portfolios: super-premium consoles for corporate hospitals and teaching institutions, versatile mid-range carts for state and district hospitals, and aggressively priced portable and handheld platforms customised for government tenders, PPP models, and outreach programmes. AI guidance, auto-measurements, and structured workflow templates are being foregrounded in cardiology, obstetrics, emergency, and critical care projects, where the shortage of trained sonographers and radiologists makes automation and consistency essential rather than optional.
Indian manufacturers are simultaneously expanding across the value and mid segments with systems built for local realities–unstable power, high patient throughput, multilingual interfaces, and minimal on-site technical support. Several domestic players are co-developing compact and POCUS platforms with software firms, embedding Hindi and regional language interfaces, simplified clinical protocols, and bundled training and certification into their offerings. This India-first design philosophy extends to total cost of ownership: machines are expected to be rugged, easily repairable, and maintainable by local engineers instead of relying solely on metro-based service hubs.
Go-to-market models are evolving in parallel. Rather than depending only on one-time capital sales, vendors are increasingly packaging ultrasound-as-a-service through rentals, operating leases, pay-per-scan options, and managed service contracts that bundle equipment, maintenance, software updates, and sometimes even remote reporting into a single recurring fee. For Ayushman Bharat and state-backed insurance schemes, both global and Indian players are partnering with diagnostic chains and hospital networks to embed ultrasound into hub-and-spoke architectures, where district and sub-district centres feed standardized scans into central reading pools backed by strict quality-assurance protocols.
Within this context, point-of-care and compact systems have become the most contested battlegrounds. Vendors are racing to place rugged, battery-backed, 4G/Wi Fi enabled platforms into emergency medical services, mobile medical units, health and wellness centres, and primary health facilities, with tele-ultrasound integration now pitched as a default promise rather than a premium add-on. Some multinationals increasingly lead not with a machine but with a program–such as an antenatal screening initiative, a TB or NCD outreach package, or a critical-care POCUS bundle–where devices arrive preconfigured with cloud viewers, structured reporting templates, and embedded training pathways for doctors, nurses, and technicians. Training and service have quietly become the main levers of differentiation: academies, simulation-based workshops, blended e-learning, and app-based microlearning are being tied closely to vendor ecosystems, while tenders and private RFPs heavily weight service metrics such as regional coverage, spare-part availability, remote diagnostics, and 95–99 percent uptime commitments. In 2025, success for ultrasound vendors in India is measured less by how many boxes they ship and more by how convincingly they can own the end-to-end ecosystem–devices, software, financing, training, service, and clinical programs stitched into a coherent, scalable story from metro quaternary centres to the last mile.
Concerns about PNDT-linked red tape throttling the market are well founded, with practitioners across multiple states reporting year plus delays driven largely by registration bottlenecks rather than lack of demand or weak returns on investment. The core structural issue is that, under sustained pressure to tighten implementation of the PC PNDT Act, many state governments have shifted appropriate authority powers upward to District Magistrates and other IAS officers, who tend to view ultrasound primarily through a sex selection lens and often lack the time or domain context to clear applications at the pace a high velocity diagnostic modality requires.
Under the Act, ultrasound clinics are effectively treated as genetic clinics whenever prenatal use is possible, and violations are cognizable, non bailable, and non compoundable, creating a compliance environment where even minor documentation errors can result in machine seizure and criminal proceedings. This has fostered a climate of fear that is disproportionate when ultrasound is used for general radiology and whole body diagnostic applications. Recent analyses by UN agencies and policy commentators note that the Centre has encouraged states to designate District Magistrates as District Appropriate Authorities, and states such as Goa have formally notified DMs as AAs under PC PNDT, adding a senior IAS layer on top of medical officers and advisory committees; in practice, uneven district level interpretations and overburdened DMs mean approvals and renewals can drag on for 6–8 months or more, even when capital has been deployed and orders placed for what is, in most use cases, a versatile, non ionising imaging tool.
From an industry and access perspective, this is a classic example of a law with sound intent but difficult–and at times perverse–consequences: medium term forecasts still project India’s ultrasound revenues growing at roughly 6–8 percent CAGR through 2030, yet PNDT compliance overheads, registration friction, and fear of punitive action are now cited as material brakes on installations, especially in small centres and anaesthesia or emergency practices that would benefit most from point of care ultrasound. A more balanced framework would retain the non bailable severity reserved for sex selection offences while restoring day to day registration powers to trained medical appropriate authorities, explicitly de linking general and multi organ ultrasound from the core PC PNDT enforcement machinery wherever feasible, and moving toward time bound, fully digital, file tracked approval pathways in which a DM or IAS officer exercises oversight rather than functioning as yet another slow, mandatory sign off in an already congested pipeline.
Collaboration – Ultrasound’s quiet accelerator
Behind every leap in ultrasound capability lies an invisible web of partnerships. Device makers now routinely team up with AI start-ups, academic labs, telehealth companies, and health systems. The goal is no longer to ship a standalone scanner; it is to deliver a clinical platform that fits seamlessly into real-world workflows.
Such collaborations do more than share risk; they compress time. Joint research accelerates the path from concept to prototype, from pilot to guideline, from niche to standard of care. When hospitals co-design systems with vendors, the resulting architectures are more intuitive, more connected, and more tuned to frontline realities–whether that means scanning a trauma patient in a crowded ER or following up a heart failure patient at home.
Funding alliances deepen this effect. Public–private investments and consortia reduce the financial burden of high-risk innovation, while ensuring that performance, safety, and usability remain central. The reward is a resilient, scalable ecosystem in which advances in one corner–say, edge AI for handheld devices–can diffuse rapidly into other segments, from cart-based systems to wearables.
Where the reinvention starts – At the probe
For all the attention on software and AI, ultrasound’s reinvention still begins with the transducer. This is where electrons become sound, and sound becomes information. Early probes were bulky, power-hungry, and limited in bandwidth. Today’s transducers, built on MEMS and advanced composite piezoelectrics, are smaller, more sensitive, and engineered like precision instruments.
This evolution has unlocked a duality that would have seemed contradictory a generation ago: systems that are both higher performance and more portable. A single compact probe can now handle superficial vessels and deep abdominal organs, thanks to broadened bandwidth and refined impedance matching. This versatility simplifies both purchasing decisions and daily practice–one device, many use-cases.
Miniaturized, flexible transducers are paving the way for something more radical – wearable ultrasound. Researchers and industry consortia are developing patches and garments capable of continuous monitoring of deep structures, from the lungs and heart to musculoskeletal systems. These devices blend advanced transducer design with bioadhesive materials and edge AI, turning ultrasound into an always-on observer rather than an occasional visitor.
When code becomes the core
If transducers provide the raw music, software increasingly conducts the orchestra. Ultrasound has entered the era of software-defined imaging, where performance no longer depends primarily on hardware revisions. Beamforming, noise suppression, Doppler processing, and image enhancement now live in flexible, upgradeable software stacks.
This shift changes how innovation feels at the bedside. A device that once required replacement to gain new capabilities can now receive an update and emerge, overnight, with sharper images, faster workflows, or new AI-assisted tools. Beam patterns can be reconfigured, post-processing tuned, and automation refined, all without swapping out the physical scanner.
It also changes how companies compete. Differentiation is migrating from incremental hardware tweaks to the quality, speed, and intelligence of algorithms–and to how well those algorithms integrate with broader digital health systems. The scanner becomes one node in a networked environment that includes PACS, EMR, clinical decision support, and cloud analytics. Hardware still matters, but software increasingly writes the story of what is possible.
AI at the probe – Guidance, not replacement
At the point where clinician meets patient and probe, artificial intelligence is quietly rewriting the script. Instead of relying solely on a user’s muscle memory and pattern recognition, smart systems now guide probe placement, suggest optimal views, adjust parameters in real time, and even confirm whether a specific protocol has been completed adequately.
This is more than convenience. For early adopters and non-experts, AI assistance shortens learning curves and reduces the cognitive load of multitasking in high-pressure environments. For experienced users, it acts as a safety net, catching missed views or subtle findings that might otherwise slip by.
On the interpretation side, AI parses pixels into metrics. It measures chamber volumes, wall motion, shear wave speeds, and vascular flow patterns with unwavering patience. Over time, it builds comparative baselines for each patient, flagging changes that point to early disease progression or treatment response. The effect is cumulative – each scan becomes both a decision point and a contribution to a growing, learning dataset that refines the technology itself.
From image to insight to foresight
The most profound change, however, is not in how images are acquired or sharpened, but in how they are used. Traditional imaging asked – What is wrong now? AI-enhanced ultrasound increasingly asks – What will happen next?
By correlating imaging features with outcomes across large populations, predictive models can estimate risk trajectories–who is likely to decompensate, which lesions will progress, which therapy is most likely to succeed. In this environment, an ultrasound exam is no longer just a snapshot; it is a data point in a predictive narrative.
This shift has practical consequences. High-risk patients can be followed more closely, therapies fine-tuned earlier, and hospitalizations potentially averted. In busy clinics, such tools help prioritize who needs advanced imaging or specialist referral today and who can be monitored safely over time. The aim is not to replace human judgment, but to stage the data so that insight is easier to grasp and harder to overlook.
POCUS and the culture of immediacy
Nowhere is ultrasound’s cultural impact more visible than in point-of-care ultrasound (POCUS). Its ethos is simple – ask focused clinical questions and answer them, where possible, at the bedside in real time. Is there fluid around the heart? Is the lung collapsed? Is the foetus alive and appropriately growing? Each answer shortens a chain of uncertainty that previously spanned multiple departments and hours.
POCUS has become a language taught in medical schools, embraced by emergency physicians, intensivists, anesthesiologists, and increasingly generalists. Its rise has not been without debate–questions around training standards, documentation, quality control, and scope of practice continue–but its momentum is unmistakable. For many clinicians, it has become as indispensable as the stethoscope, and arguably more informative.
As AI and tele-ultrasound strengthen POCUS, its reach expands beyond specialists. Rural doctors, paramedics, and community health workers can access expert guidance remotely while performing scans locally. In humanitarian crises, handheld devices help distinguish who must be evacuated urgently from who can be treated on site. The result is a subtle but profound redistribution of diagnostic power.
Frontlines, fault lines, and real-time resilience
In the harshest environments–earthquake zones, epidemic outbreaks, combat theatres–ultrasound often serves as the only viable imaging option. Its portability, lack of radiation, and ease of sterilization make it uniquely suited to chaos. Paired with satellite or mobile connectivity, it becomes a lifeline connecting frontline responders to radiologists and specialists hundreds or thousands of kilometres away.
Yet these contexts expose fracture lines too – devices must survive dust, humidity, jolts, and makeshift power supplies. Connectivity can fail at crucial moments. Operators may be minimally trained and under extreme stress. The push now is to design systems that anticipate such realities – rugged casings, offline AI triage capabilities, data caching, and workflows that prioritize resilience over elegance.
In this sense, ultrasound has become a litmus test for health system adaptability. Where it is integrated thoughtfully–into protocols, logistics, and training–it enhances resilience. Where it remains an afterthought, its potential is blunted by the very constraints it was meant to overcome.
The rise of always-on ultrasound
One of the most intriguing chapters in ultrasound’s reinvention is being written not in radiology but in research labs working on wearables. Here, ultrasound is shedding its identity as a device you bring to the patient and becoming a presence that stays with the patient. Patches that adhere to the chest, abdomen, or limbs can now capture continuous images or measurements over hours or days. Projects like SonoSkin in Europe and bioadhesive ultrasound platforms in Asia illustrate how MEMS-based transducers and edge AI can support deep-body monitoring outside the lab.
For patients with heart failure, lung disease, or high-risk pregnancies, this opens a radically different model of care. Instead of waiting for symptoms to reach crisis levels, clinicians can track trends in function and intervene earlier. For athletes and workers in high-stress environments, continuous musculoskeletal monitoring may help prevent injury rather than simply diagnose it afterward.
As clinical trials scale up, questions of data volume, interpretation responsibility, reimbursement, and patient comfort will come to the fore. But the direction of travel is clear: ultrasound is stretching from an episodic test to a continuous presence in the patient’s health story.
Hands-free, not hands-off – Robotics and autonomy
Another frontier lies in robotic and autonomous ultrasound. Here, the aim is not to remove clinicians from the loop, but to free them from geographic and physical constraints. Robotic arms, guided by remote experts or AI, can reproduce standardized sweeps, maintaining consistent pressure and angles that human operators might find hard to sustain–especially in repetitive or high-risk procedures.
In intensive care units, autonomous systems could one day perform routine lung or cardiac scans at scheduled intervals, feeding data directly into monitoring dashboards. In remote clinics, a nurse could position a robotic probe, while a specialist hundreds of kilometres away controls fine movements or confirms the adequacy of images.
Each step toward autonomy raises important questions about accountability, safety, and ethics. Yet it also offers a path to scaling the benefits of expert-level imaging without requiring an expert at every bedside. The likely endgame is a hybrid model in which human judgment and machine precision complement one another rather than compete.
Ultrasound as therapy – From witness to actor
Ultrasound’s reinvention is not confined to seeing; it increasingly includes doing. Focused ultrasound now treats essential tremor and certain tumours, dissolves clots, and modulates neural circuits in carefully targeted regions. In cardiology, acoustic energy can help address calcified plaques or support transcatheter interventions, reducing the need for open surgery.
Low-intensity therapeutic applications are more subtle but equally promising–nudging cells toward regeneration, modulating inflammation, or helping drugs cross barriers that would otherwise limit their effectiveness. Even implanted devices, long plagued by biofilm formation and mechanical wear, may benefit from periodic ultrasound maintenance that extends longevity and reduces the need for replacement surgeries.
These therapeutic uses deepen ultrasound’s integration into care pathways. The same modality that detects a lesion may eventually help treat it, monitor the response, and guide long-term follow-up. The line between diagnostic and therapeutic platform grows thinner with each new indication.
3D, 4D, and the power of seeing whole
Clinicians have long been adept at mentally reconstructing three-dimensional anatomy from two-dimensional slices. Real-time 3D and 4D ultrasound relieve some of that cognitive burden. In structural heart disease, obstetrics, and interventional radiology, volumetric views clarify spatial relationships that are difficult to grasp in flat planes.
These models also extend beyond the moment of the scan. Digital twins of valves, foetal hearts, or vascular anomalies can be manipulated, rehearsed upon, and used for training. Residents and fellows can walk through complex anatomy repeatedly before ever entering an operating theatre. In the room, live 3D guidance offers a second pair of eyes that never tires, continuously updating as catheters move or anatomy shifts.
The emotional impact is not negligible. For patients and families, seeing a heart valve or foetus in three dimensions makes conditions more tangible and treatments more comprehensible. It invites them into the decision-making process in a way flat images rarely do.
Fusion imaging – When one view is not enough
In the most complex cases, no single modality tells the whole story. Fusion imaging acknowledges this by overlaying real-time ultrasound on pre-acquired CT, MRI, or PET data. The result can feel almost like augmented reality – an interventionalist sees not only the live needle or catheter tip, but also the context of prior imaging, metabolic activity, or lesion margins all at once.
Yet achieving such harmony has not been easy. Early systems struggled with misalignment due to patient movement, breathing, or minor differences in probe positioning. Manual registration demanded time, skill, and a tolerance for imperfection.
Today, AI-driven registration, phantom-based validation, and rigorous quality assurance are gradually taming these challenges. As workflows mature and training spreads, fusion imaging is moving from advanced option to expected capability in high-end systems–especially in oncology, hepatology, and complex vascular interventions. The promise is simple – fewer surprises, more precision, and greater confidence at critical junctures.
Trust – The invisible currency
Amid all this change–physics, AI, robotics, therapeutics–one element remains non-negotiable: trust. Clinicians will only lean on tools they believe to be accurate, transparent, and consistent. For ultrasound, that trust must be earned and re-earned through robust validation, post-market surveillance, and clear communication about how algorithms were trained and how they behave in the wild.
Quality assurance becomes the quiet backbone of adoption. Phantom testing, inter-operator comparisons, and outcome audits help ensure that performance on paper translates into reliability at the bedside. Transparent reporting of limitations, failure modes, and edge cases makes it easier for clinicians to use the technology wisely rather than blindly.
When trust is present, technology recedes into the background and clinicians focus on patients. When it is absent, even the most advanced systems risk sitting unused, their promise stranded between skepticism and uncertainty.
Commercial pathways – From machines to ecosystems
Commercial success in ultrasound increasingly depends on seeing beyond machines. Health systems no longer want isolated boxes; they want ecosystems that integrate with existing IT stacks, align with reimbursement realities, and adapt to local workforce skills. Subscription models, cloud-based analytics, and service-driven offerings are replacing one-time capital purchases in many regions.
For vendors, this means thinking in platforms rather than products. A handheld scanner may be bundled with AI-guided training, tele-ultrasound access, and integration into national screening programs. A high-end console might anchor a multi-hospital network, feeding anonymized data into research pipelines while pushing back decision support in near real time.
This ecosystem approach also opens space for new entrants and partnerships. Start-ups specializing in niche AI tools can plug into larger platforms, while local integrators can tailor global technology stacks to regional realities. The companies that thrive will be those that pair technical innovation with empathy for the everyday frictions of clinical work.
The 2030s – Ultrasound as a living system
By the 2030s, ultrasound will likely look less like a category of machines and more like a living system threaded through healthcare. A continuous loop will connect transducer, algorithm, clinician, and patient record. Every scan will not only inform a single decision, but also add to a shared pool of knowledge feeding future algorithms and guidelines.
In that world, the value of ultrasound will be measured less by pixel quality and more by the quality of outcomes it helps to deliver: earlier diagnoses, fewer unnecessary procedures, safer interventions, more personalized therapies. Precision medicine will depend not just on genomics or lab data, but on richly annotated imaging streams that capture the dynamics of disease over time.
The reinvention that began with better crystals and clever beamforming will culminate in something broader–a truly intelligent clinical platform woven into the fabric of everyday care. Ultrasound will not merely show what is happening inside the body; it will help decide what should happen next, and when, and for whom. And in that quiet but radical shift, the story of ultrasound becomes inseparable from the story of modern medicine itself.